
When her sister was diagnosed with breast cancer in her thirties, Julia Mack, RN, BSN, knew she should get genetic testing. Ms. Mack’s sister had tested positive for an inheritable breast cancer gene, and other family members had been affected by cancer at relatively young ages.
Despite this, Ms. Mack, who is nursing team lead at the UHS Breast Center, says she procrastinated a bit; she had reason to believe she didn’t have the gene based on her individual health history. This kind of stalling is not uncommon, she says. It’s something she’s witnessed among her patients as well. “We tend to be in denial about cancer, but it can be so helpful to know all the factors that can affect your risk level.”
Ms. Mack, who is 42, did test positive for the BRCA 1 gene, which she and her sister have inherited from the paternal side of their family. The gene makes women and men more susceptible to breast and other cancers, such as ovarian and prostate cancer, at an early age.
While it wasn’t the news she’d hoped for, Ms. Mack says this knowledge helped her to take potentially lifesaving steps to prevent cancer and to catch it early if it occurs. It will also allow her daughters and son to make more informed choices about their own screening and prevention steps as they move into their twenties. “It’s something that affects all of these decisions,” she says.
WHERE TO START

Jennifer Schecter, FNP-BC, OCN
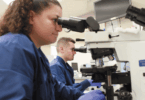
While genetic mutations like BRCA are rare, there are many other factors, such as lifestyle, health history and breast tissue type, that can help determine a woman’s breast cancer risk. Knowing what factors affect you and what your risk level is can point you toward the most helpful preventive steps, as well as the most effective screening schedule, says UHS High Risk Cancer Clinic Specialist Jennifer Schecter, FNP-BC, OCN.
For many women, the first step in determining risk is a conversation with a primary care doctor. Your doctor can perform a manual breast exam, record relevant facts about personal and family medical history, address questions about mammogram recommendations, and refer you to further testing or consultations with a specialist if needed, says Ms. Schecter.
Details of a family history of cancer, including type of cancer and age of onset, can be very helpful in determining risk level, as is familiarity with your own breasts, Ms. Schecter says. “Some women are uncomfortable with self breast exams, but recognizing any changes, such as an unfamiliar lump, skin changes or nipple discharge, is very helpful information for your doctor.”
Women who are found to be at average risk can typically follow standardized screening recommendations, which may include a yearly mammogram, depending on age. Those at high risk may have more frequent mammograms, or doctors may recommend using additional breast cancer imaging technology, such as ultrasound or MRI.
In addition, some women and men with a strong likelihood of inheritable cancer may benefit from genetic testing. At the UHS High Risk Cancer Clinic, women can discuss their options and be referred to a genetic counselor when appropriate, says Ms. Schecter. If a genetic test is recommended, it will typically consist of a simple blood or saliva test.
PREVENTIVE MEASURES
What you choose to do with your risk knowledge is a very personal decision, says Ms. Schecter. In Ms. Mack’s case, once she found out she had the BRCA 1 gene, she consulted with her doctors and decided to have her ovaries and fallopian tubes removed, a procedure that is known to significantly reduce the likelihood of breast and ovarian cancer, she says. Going forward, she will follow high risk screening guidelines, including annual mammograms and MRIs, six months apart from each other.
Ms. Mack says she’s grateful that she and her sister can benefit from the knowledge, testing, prevention and treatment methods that weren’t available when her relatives faced cancer years ago. “We knew we had a family history, but until recently there was no way to know the role genetics played. It’s amazing how far we’ve come,” she says.
NEW SURGEONS SPECIALIZE IN BREAST HEALTH
Two new surgeons have joined UHS. With the addition of these highly-trained physicians, UHS can expand access to the latest in surgical techniques for women with suspected or diagnosed breast cancer, from biopsy through reconstruction.
Board-certified breast surgeon Colleen O’Kelly Priddy, MD, has joined the UHS Breast Center. She received her Doctor of Medicine from the University of Nevada School of Medicine and completed her residency at University of Washington Affiliated Hospitals. She completed a fellowship in Oncologic Breast Surgery at the University of Southern California.
Plastic surgeon Omotinuwe Ife Adepoju, MD, has joined UHS Plastic Surgery. Dr. Adepoju completed her medical training at Weill Cornell Medical College and her residency at Rutgers University Robert Wood Johnson University Hospital. Her fellowship training took place at the University of Minnesota Medical Center.
GET CHECKED
Visit UHS Breast Care to learn more about resources at UHS and to schedule a mammogram at a UHS location near you.